For many runners the first sign of an Achilles injury “comes out of nowhere” as they take their first steps in the morning. As we sleep the feet are pointed and the calf muscles tighten up making it feel as if we’re walking with blocks of wood on the ends of our legs. As athletes we tend to ignore minor aches and pains as consequences of an active lifestyle, however many of the warning signs of impending Achilles issues are there, if we look for them.
Firstly, we need to distinguish from an –itis and an –osis. When you see the phrase tendonitis it infers that there is inflammation of the tendon by micro tears through overloading. This is entirely different to a tendinosis, which is a breakdown of the structure of the tendon in response to chronic overuse. While both present as pain the treatments for both are different, and it is important to make sure the diagnosis is correct. To further complicate matters it is also possible to have the pain caused by where the tendon itself runs through the sheath. Again, treatment is different for an Achilles issue – either micro tears or degradation – versus an Achilles tendon sheath issue.
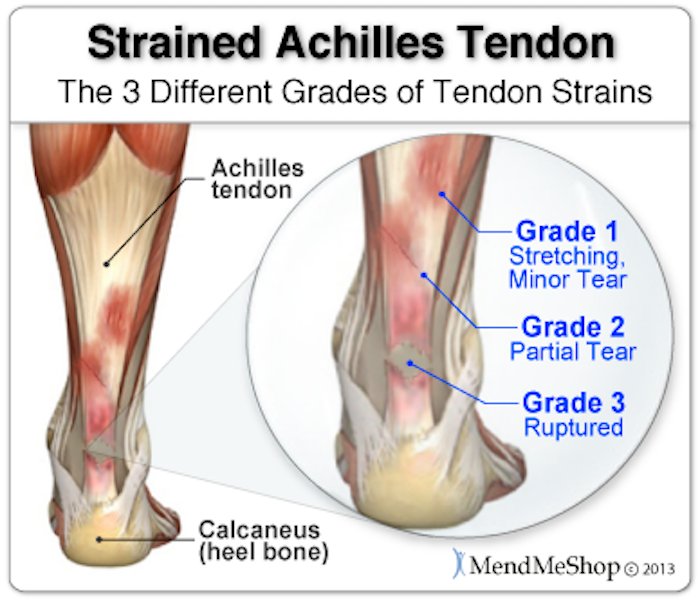
A final issue that can occur is the complete rupture of the tendon itself. Trust me when I say this – if your Achilles tendon snaps you will not be left in doubt. You will fall to the ground as if shot by a sniper. Recovery from a complete rupture will require reattachment or repair surgery and will be around twelve months before you can even be ready for regular training again.
Achilles issues, both –itises –osises, are simple to detect. Pain will be localized to the area of the Achilles tendon. If you pinch the area between thumb and forefinger you’ll find it incredibly tender. A partial tear of the tendon will feel the same way so you’ll need a professional diagnosis and scans to differentiate. However, a complete tear will be obvious as there will be a gap in the tendon and you’ll be unable to walk with normal gait on the affected side.
Over the last decade or so there has been a considerable change in the understanding of Achilles injuries, which has followed from the finding by Khan et al. (1999) that inflammation (tendonitis) isn’t present. On microscopic examination it has become evident that the collagen structure itself has begun degenerating and that scar tissue has begun forming. My belief is that many patients suffering from Achilles issues worldwide are being diagnosed incorrectly and therefore treatment for their issue, which never seems to go away, is also wrong.
Peak age for Achilles troubles are between 30 and 50 years old. Given most of the problems are to do with degeneration of the collagen structures, and this occurs as we age, it is natural that the issue should be evident in ageing runners. There are studies to show that runners who have run far and fast are most likely to suffer from these problems compared to others who either take up running later or who have not pushed the limits as much.
One of the possible causes is that we tend not to use the muscles for propulsion as we run, but tend to bounce off our tendons. There is a correlation between age, how much stretch can be achieved in the tendons due to loss of collagen, and running speed.
There are other factors though, usually cited as: tight, inflexible calf muscles; hypermobile feet; and overly stiff feet. In other words – every single person who runs may get Achilles tendinosis. Having suffered from Achilles tendinosis for a period leading into Ironman – brought on by a big increase in mileage – I’ve been through all the tests and treatments you could imagine. My feet are stiff, and the calf is forced to take the brunt of much of the shock absorption that my feet won’t.
Looking back what strikes me as odd is that not one therapist did much other than offer me what amounted to a band aid to treat the issue. One therapist did some great work on breaking up my feet so that they were more flexible, however, there was no plan in place to try to make my feet more flexible long-term. Just this idea that my feet were stiff and they would remain that way forever.
Tendon problems should be treated with care as they can quickly go from an –itis to an –osis, meaning that long-term damage has been sustained. Immediately at the realization that there is pain in the area rest must be taken. However this shouldn’t be a few days, or even a few weeks, but is much better as a few months. I know this is painful news for runners (excuse the pun) but isn’t it better to take a few months now rather than risk not running altogether in a year or so?
Studies have shown that eccentric strength training in the calf muscles is an effective way to rebuild tendon cells. Work on these heel lowering exercises should already be in the arsenal of all runners, but if they’re not they need to be immediately added in if these issues arise. These same studies have shown that in injured runners eccentric calf strength – the strength that stops your foot slamming into the ground on each step and helps you absorb the impact forces – is lower than in healthy runners.
Remember that an inflammatory condition – actual tendonitis – will settle in three to six weeks. Anything that takes longer is not an –itis, but has formed into a degrading condition and needs to be addressed differently. Given that the majority of Achilles problems are not inflammatory the use of ice and anti-inflammatory drugs such as ibuprofen, etc. is unproven as part of a treatment plan.
The first step has to be to limit or stop running immediately. My personal preference with people is that at the first signs of soreness in the area that the runner is rested for anywhere from one to three weeks. During this time use activities that do not load the Achilles as much such as cycling and swimming, although you may need to alter cleat position for riding to prevent any further damage being done, and you’ll also need to make sure to only ride sitting as standing may make it worse too.
A note on cortisone injections into an area that is suffering from a tendinosis. Given the condition is one of degradation and a cortisone injection is designed to breakdown tissue to prevent further inflammation it is entirely possible that a cortisone injection could make the Achilles more likely to rupture in the injection site.
Like with most of the injuries discussed, keeping it in stage 1 is vital if you are keen to resume running soon. Injuries that are managed well in stage 1 do not usually linger and no great changes need to be made to training plans. One thing I have found particularly useful for myself as well as those I train who have also been down this path is to never wear minimal shoes. Many “functional” trainers these days get their clients to wear barefoot or wearing minimalist footwear with zero drop soles. In my experience this puts the calf and Achilles on stretch all the time, not just during running and stops it healing quickly. The best bet is to find a shoe that you can lift weights in that has a bit of a heel, but that isn’t too cushy. This allows the calf/ Achilles to relax a little when not running. For me, this little change allowed my Achilles to go from painful to pain free in just two weeks.
Noakes has this as a guideline for Achilles problems in Lore of Running:
Stage 1 (morning discomfort in tendon)
Rest one week before resuming running training as before.
Stretch calf muscles for a total of 20 minutes daily.
Try new running shoes that prevent pronation.
Add 7 to 15mm heel rise to running and street shoes (either by using shoes with higher heels or by using inserts).
Monitor injury progress with pinch test.
Use physical therapy and drug therapy if costs permit.
Stage 2 (pain during running, but not affecting performance).
Continue approach for stage 1.
Modify training to reduce speed work, hill running (particularly downhills) long runs, and weekly distance.
Try an orthotic.
Physical therapy.
Stage 3 (pain during running that is affecting performance).
Continue as for stage 1 and 2.
Rest for 3 weeks.
Try regular cross friction massage to break up scar tissue build up in area.
After 3 week rest, resume jogging, cycling, swimming (no serious running) until injury reverts to grade 2, then try serious running only when injury reverts to grade 1.
Stage 4 (running impossible)
Try approaches for stage 1, 2, and 3.
If these fail, visit an experienced orthopedic surgeon.
Consider surgery only when all other techniques, including repeated sessions of cross-friction massage, have not worked.
(The following comments and suggestions are by Greg Dea, one of the world’s leading sports physiotherapists).
Often, the tendon pain occurs after a temporary increase in tendon loading, for example – increase in speed, volume, frequency of running, or even something as sneaky as running on a cambered surface, like road running where the road slopes a little to drain water, then when you run back home, you cross the road only to end up having the same camber. Be careful also of the “usual run” that has no change in any of those parameters, but follows on from a period of stress in other ways, eg. When you’ve not fully recovered from a fatiguing event. Here’s the responsible advice – don’t be the person whose Achilles tendon pain comes from a medical problem where a fitness solution isn’t right. A quick check with your responsible health practitioner is the first step.
The good news is that tendons don’t like to be rested, so you’re not going to be expected to simply not do anything. They don’t get better with rest, they get better with modified load. They get better with better movement and better load tolerance in other parts of the body. They will, however, benefit from direct treatment, so get ready to step up and help your little buddy.
In the Functional Movement Systems, one of the principles that guide clinicians and coaches through injury and movement problems is the three steps paradigm of Reset, Reinforce, and Reload. This applies to Achilles pain too. The Reset means when someone does something to you that removes pain or restores movement you couldn’t do yourself. With advances in self-help, we can use many tools to reset ourselves.
When it comes to pain in the tendon, for mine, it comes down to whether you have just had pain in the last 24 hours, or whether it’s been hurting beyond 2 days.
If it’s a fresh Achilles pain, within a day, the active ingredient in simple over-the-counter medicine Ibuprofen has been shown to quieten down the tendon cells that spew out a different water-attracting-protein – the reason for the swelling. You’ve got to block these cells right away – if you miss using ibuprofen straight away, you’ll have missed the opportunity to minimize the tendon swelling in the short term.
If it isn’t a fresh Achilles tendon pain, the biggest bang-for-buck thing you can do is consider, with your local doctor who’s experienced in sports injuries, the use of GTN patches. GTN, or Glycerol Tri-Nitrate, is usually used to treat angina, as it releases nitric oxide, which opens blood vessels. It’s not clear why opening blood vessels helps Achilles tendon pain, but it certainly does. So many of my Australian Football player athletes with Achilles tendon pain have had their pain abolished within a couple of weeks – if you think that’s a long time, it’s not – these tendons can be painful for weeks to months. You’ll need a prescription from your doctor, who should be familiar with its use in Achilles tendon injuries. If your doctor doesn’t know about it, go to one who does, or provide them with this article to study.
For more comprehensive information on running and how to cope with and treat the most common injuries get your copy of Run Strong here.